
 The Other Side
The Other Side
The next step seemed to be to look at what literature MANA had neither generated nor opted to include in their list of “best evidence.” MANA had not provided me with a handy list of opposing information, so I needed to search it out myself.
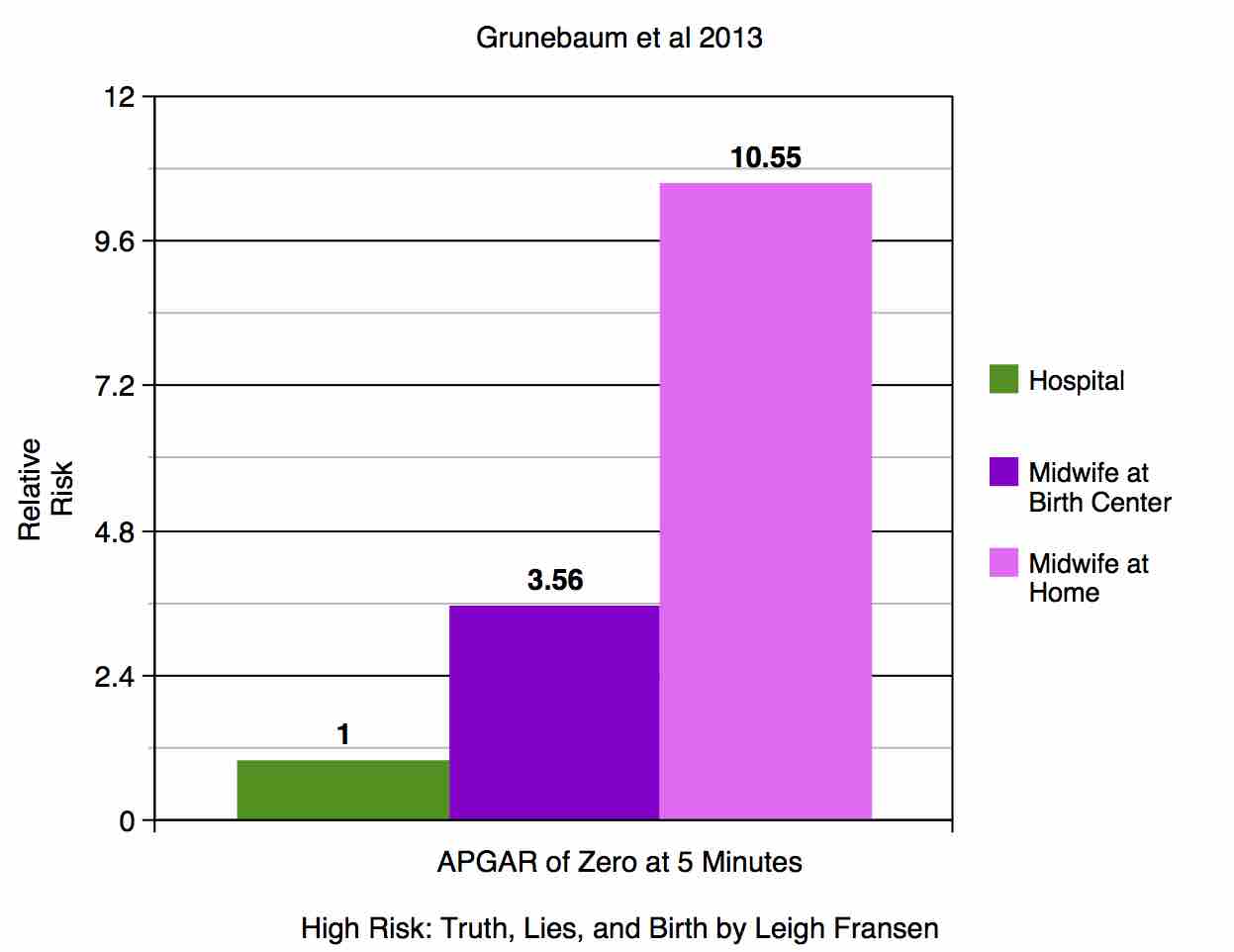
Grunebaum et al 2013: The American Journal of Obstetrics & Gynecology addressed choice of birthplace twice in October of 2013.
The first, “Apgar score of 0 at 5 minutes and neonatal seizures or serious neurologic dysfunction in relation to birth setting,” by Grunebaum et al, was the first to examine birth setting by the outcome of a zero Apgar at five minutes. The Apgar score is assigned to every baby at one and five minutes of life, regardless of birthplace, as long as the attendant is trained to assign one. The score is reported on birth certificate data. A “perfect” score of ten indicates a baby that is vigorous, well-oxygenated, and transitioning very well to extrauterine life. A baby with an Apgar score of 0 at five minutes essentially means the baby had no signs of life at that time; a baby with no signs of life at 5 minutes of age may or may not survive, and if they do they will likely suffer from severe brain damage. This study found that babies had 3.56 times the risk of Apgar 0 at 5 minutes when born with midwives at a birth center, and 10.55 times the risk when born with midwives at home. Nonhospital births also carried significantly higher risk of neonatal seizure or serious neurologic dysfunction.
It is important to address the fact that the use of birth certificate data is not perfect. First of all, although hospital births always include the filing of birth certificate data, the same cannot be said of all home births. Especially in states where midwifery is illegal, midwives do not always fill out or submit birth certificate data. The parents will often submit the birth certificate paperwork themselves, and may or may not submit an Apgar score with any accuracy. Secondly, when a woman is transported to the hospital during labor because something isn’t going right at a planned nonhospital birth, the hospital has no way of indicating on the birth certificate data that the birth was an aborted home birth attempt. Therefore, the data on hospital deaths includes most homebirth transfers that ended in tragedy. Those babies are recorded as hospital deaths or grave injuries and not as nonhospital deaths or grave injuries. Thus, it is not only likely, but assuredly the case, that these numbers for neonatal mortality are underestimating the number of deaths and injuries to babies that can be attributed to planned nonhospital birth, perhaps drastically.
Cheng et al: In the same issue of AJOG, Cheng et al published an analysis of the CDC data that focused on low 5-minute Apgar scores at two thresholds, below four and below seven, as well as neonatal seizure. Cheng found that babies born at home had a nearly two-fold increased chance of a five-minute Apgar below four, and over twice the chance of a five-minute Apgar below seven. Cheng also found that the chance of neonatal seizure was over three times higher in the home birth group. Cheng reported that women who give birth at home are much less likely to experience obstetric interventions such as antibiotic use, induction of labor, and the use of vacuum or forceps-assisted delivery. The paper concluded that planned home births resulted in a trade-off, with fewer obstetric interventions received but a significantly increased chance of neonatal complications.
Grunebaum et al 2014: In January 2014, Grunebaum et al took another look at birthplace safety and published an analysis of CDC data not unlike the informal one I did for this paper. They found that hospital midwives had a neonatal death rate of .31/1000, a number strikingly similar to Janssen’s Canadian homebirth numbers discussed earlier. Midwives working in a nonhospital birth center had a neonatal death rate of .63/1000, double the rate of death compared to the hospital, and home birth midwives had a neonatal death rate of 1.32/1000, over four times the risk of neonatal death compared to the hospital midwives. Grunebaum’s findings can be further expressed by explaining that for every 10,000 babies born at home with a midwife, about ten will die a death that would have been preventable in the hospital.
Rooks: With this literature arising from the obstetric world, the reader may wonder if any midwives had noticed a similar trend. I was able to find one who had: in 2013 a Certified Nurse Midwife in Oregon named Judith Rooks not only identified the trend, but submitted a report to the state legislature detailing her findings. She found that nonhospital births with direct-entry midwives in Oregon carried six to eight times the risk of perinatal death compared to hospital births. She ended her letter to the Oregon legislature in a poignant fashion: “In 2012 six Oregon mothers lost their babies in births attended by DEMs. They may feel guilty about having chosen a home birth with a DEM and are unlikely to lobby their legislators. The more than a thousand women who had good outcomes and are happy are the ones who will call you… Please keep the six women who lost their babies last year in mind as you legislate this year.”

I am really enjoying your blog! I find your posts are easy to read and do not seem particularly biased like some other blogs I have read. I would just like to point out one other thing about birth certificate data: you mention that home births gone wrong resulting in intrapartum transfer are classified as hospital births (thus making hospital data look worse). The same could be said for unplanned homebirths, right? For instance if a mother who had no prenatal care & then delivered at home, that would be considered a homebirth? Because that would also skew the data…
That’s a great question, Ocuinn! The way researchers exclude unplanned home births is by selecting for attendant type as well as birthplace. If a midwife was present at a home birth, we can reasonably assume that it was planned, right? Unplanned home births don’t have “midwife” checked as attendant. If you would like to see all the variables available from birth certificate data, you can go to the CDC website and play around with the WONDER database yourself. It’s freely available to anyone. The database you want to select is the linked birth/death records. If you enjoy numbers, you can spend all day playing on that thing.